Follow Up Scans & Dry Mouth
The latest follow up visit to MD Anderson from 10-12 February 2026 continued the series of good news. In summary, the MRI scans remain clear, and there are no signs of tumor. In fact, the news was so reassuring that the doctors are moving me a 6 month follow up interval (vs. 3 months), so I’ll only be going to Houston and MDACC twice a year until 2028. Assuming all goes well, at 5 years post-treatment, I’ll then be on an annual follow up interval.
The visit schedule was similar to my prior itineraries: arrive on Tuesday, have an MRI scan; and then consult with the doctors and speech pathologists on Wednesday (and Thursday). As mentioned before, the scans and doctor consults are now more routine, with “boring” and “unremarkable” being the goal. The more actionable and impactful elements now focus on swallowing and rehab programs.
One interesting observation about the MRI is how busy and efficient MDACC is. My MRI was scheduled for 8:45pm on a Tuesday night at the Radiation Outpatient Center (ROC). I believe this facility does scans from 6am to 11pm. They are so busy that my last two scans there have taken place in the mobile units. ROC added these three mobile units - essentially trailers - outside the permanent building to meet demand. It is a little strange to walk out to these mobile units, as the area doesn’t feel permanent; it is tented with visible ventilation. I also have to take a lift gate up a few feet to enter the MRI unit. ROC is not the only location to get an MRI - I think MDACC has nearly 40 MRI scanners across its campus.
Oncology
I was fortunate to get the good news of the clear scans early on Wednesday, when meeting with Jill, Dr. Maniakas’s PA (Dr. Maniakas was out that day). With no symptoms or concerns and no signs of recurrence from the scan, there wasn’t too much to discuss. I haven’t thought about the thyroglossal duct cyst excision for a while and the scar is barely noticeable now. I didn’t discuss the hole in my eardrum, as that is usually addressed by a different ENT doctor at MDACC.
Dr. Faye Johnson is my new medical oncologist, following Dr. Gillison’s departure (I had met with a covering doctor during my last visit in Nov). The consultation was similar in the sense that there wasn’t much new to discuss. A welcome development was the change in the follow up schedule. Since I had only just finished my immunotherapy treatment in December 2025, medical oncology had wanted to see me on a 3 month follow up schedule. But Dr. Johnson said that she was comfortable moving me back to a 6 month schedule, which is in line with Dr. Phan’s schedule. So instead of my next visit in May, I won’t be back until August.
Dr. Johnson did confirm one encouraging bit of news. I had seen a story about Dr. Gillison (my former and trusted medical oncologist and a giant in her field) receiving the VinFuture Prize in December 2025. There was a picture of her onstage in Hanoi with her fellow laureates. Even though the reason of her leave isn’t public, it’s good to know that she is still making public appearances.
The visit with Dr. Phan and his team was similarly positive. He remains very pleased with the scans and how the surrounding structures have remained intact. Perhaps the most memorable part of the visit was when I was meeting with Dr. Kouzy, a fourth year resident. While on the phone with Aiday, Dr. Kourzy and I discussed options for how to relieve dry mouth. He mentioned a number of methods, including acupuncture, ginger chews, sugar free gums, xylitol. Unprompted, he also mentioned that sour candies may be helpful. So he confirmed what I’ve been saying all along - I NEED to buy and eat sour gummi bears for medical purposes, on doctor’s orders!
Some of the products I use to help with dry mouth
Speech Pathology Appointments & Modified Barium Swallow Study Results (from November 2025)
In addition to the oncology appointments, I had three visits related to my swallowing and speech. The first was with Dr. Aponte-Wesson, my oral oncologist. I’ll write more about that visit in a separate post. The next two were with the speech pathology team.
I met again with Dr. Barbon, who I hadn’t seen since December 2024. Her focus is on maintaining my tongue and swallowing functions. She told me that since my hypoglossal nerve has damage from radiation, there is asymmetry in my tongue strength. Specifically, the right side of my tongue is weaker than the left. That means that when I stick my tongue “straight” out, it deviates to the right (the weaker/damaged side). This happens because the left side tongue muscles push my tongue more strongly towards the right and the right side muscles cannot oppose in equal measure. The weakness also presents in pushing out my cheeks - I can’t push out as much on the left side.

My tongue deviates to the right and has asymmetric strength due to the damage to the hypoglossal nerve from the 2018 radiation
Dr. Barbon and I also discussed the swallow study from November 2025 and how it compared the previous one from March 2024. The hope was that the filler injection might be beneficial. Unfortunately, the results of the MBS showed that my swallowing is getting slightly worse. I am now at DIGEST 3 (S2, E3) “severe pharyngeal dysphagia”, which is a progression from DIGEST 2 (S1, E3). The Safety part of the score increased but Efficiency was unchanged. In summary, Safety refers to the risk that food/liquid enters the airway (Penetration–Aspiration Scale (PAS)) while Efficiency refers to strong my swallow muscles function, as measured by residue left by liquid, pudding, crackers. The report also notes “pharyngeal contraction bilaterally weak” (meaning weak swallowing muscles on both sides).
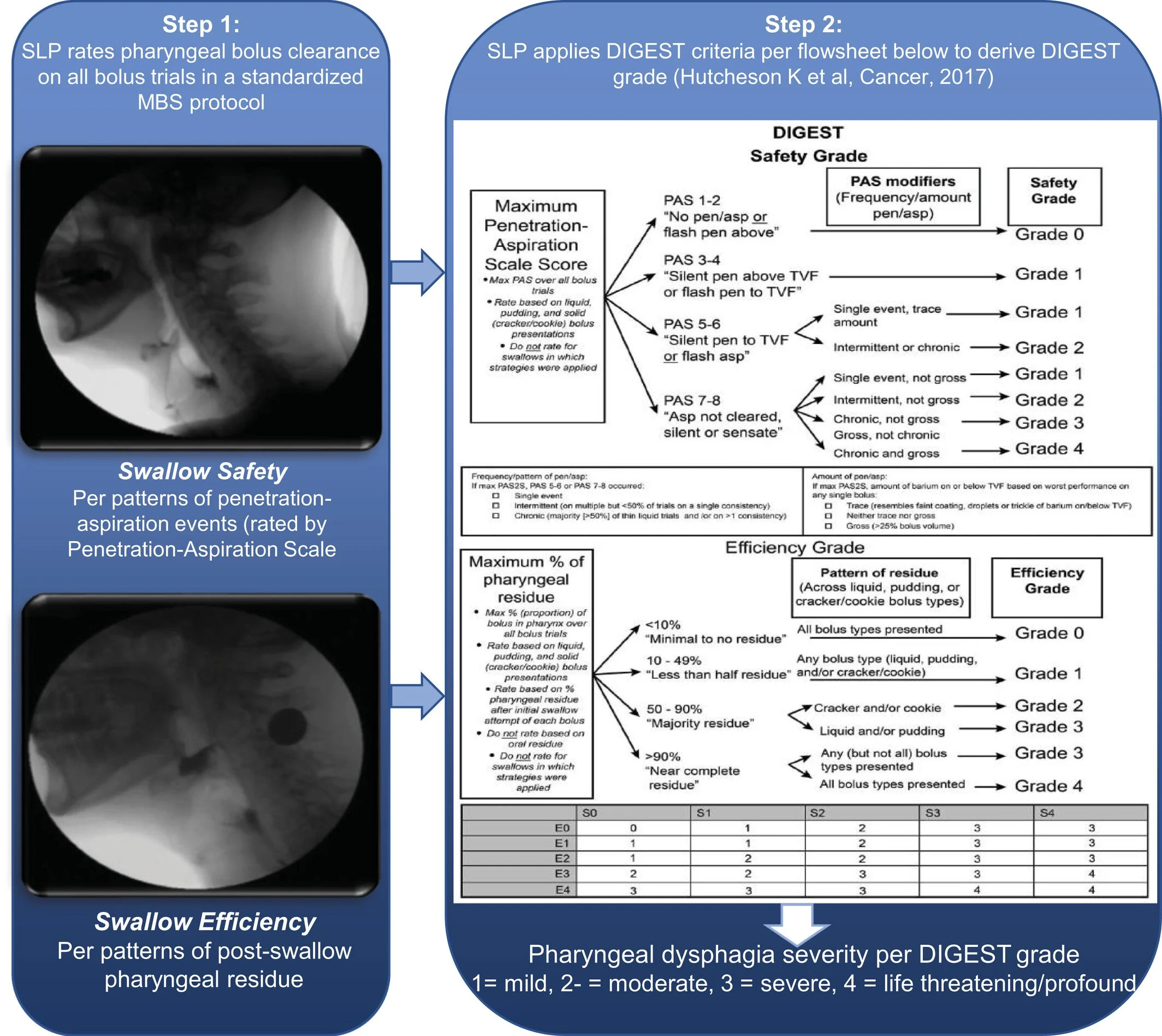
Description of DIGEST score, developed by Dr. Hutcheson at MDACC.
Hutcheson KA, Barbon CEA, Alvarez CP, Warneke CL. Refining measurement of swallowing safety in the Dynamic Imaging Grade of Swallowing Toxicity (DIGEST) criteria: Validation of DIGEST version 2. Cancer.2022. https://doi.org/10.1002/cncr.34079
Overall, while these results are clearly sub-optimal, it hasn’t yet taken away my enjoyment of food and eating. Clearly, there are some foods that are more challenging to eat, and I have to eat in a different way (more slowly, mindful of nasal regurgitation, etc.). But I can still enjoy the flavors and go out to eat without much restriction or requiring supplements.

TonguePress, IOPI and EMST devices (clockwise, from top) for my speech & swallow program
The goal of the SLP program is to maintain my function at these levels for as long as possible. Towards that end, I have several different rehab exercises to address various issues. Here is the current protocol for the week:
EMST (Expiratory Muscle Strength Training) - swallow muscle strength
Maintenance: 5 sets of 5 reps, 3x/week. Maintain highest resistance setting
Pinch nose (vs. using nose plugs) to ensure no air escapes. Do no allow cheeks to puff
IOPI (Iowa Oral Performance Instrument) - tongue strength
Maintenance: 1-3 sets of 10-20 reps (3 second max pressure hold), 3x/week for both Anterior and Posterior
For Anterior, focus on using the tip of the tongue and do not involve jaw muscles
Measurements for 1 rep max - slight decline from November 2025
Anterior: 28-35 using tongue only. Down from 36-38
Posterior: mid 30s vs 38-41 in Nov
TonguePress - tongue endurance
Endurance: hold pressure for as long as possible (12+ seconds) until failure, rest, and repeat
Measurements: was able to hold for 30+ seconds
Lingual Range of Motion - tongue deviation
With tongue out, move from side to side. Consciously initiate the movement with the weaker side
Pull my tongue to the roof of my mouth
Swallow Exercises
Four different exercises - Effortful; Mendelsohn; Supraglottic; Masako
Maintenance: 1 set of 10 reps, 3x/day, every other day
Jaw and Shoulder Mobility Stretches
A number of stretches, usually at 3x 30-40sec holds per side. 3x per week
This is to address the diminished range of motion related to the spinal accessory nerve damage
Other Side Effects
In addition to the swallowing and tongue issues, there remain other long-term side effects need to be managed, principally: i) dry mouth and gingivitis; ii) lymphedema.
Dr. Aponte-Wesson noticed more pronounced gingivitis. (I’m not sure it would have been as noticeable if I had had a recent dental cleaning, as my next cleaning is coming up shortly.) She attributed the gingivitis as a consequence of dry mouth. The constant lack of saliva in my mouth has detrimental effects on my oral health, so I’ll have to redouble my brushing and flossing efforts. She said that the xylitol lozenges and gums that I use to provide temporary relief doesn’t help for the purposes of oral health. I’ll see what my dentist say when I see them for my next cleaning.
Another issue that has resurfaced is lymphedema, particularly under my chin. A few of the doctors noticed that area feeling a little tighter, so I’ll have to re-learn how to do self massage to drain the lymph nodes and prevent it from getting worse. Fortunately, both the lymphedema and fibrosis in my neck are relatively mild, so things could be a lot worse, particularly given that I’ve gone through two courses of radiation.
That’s it for this belated update. I’m planning to provide a more detailed discussion of eating issues and the obturator soon. Thank you again for reading and for your support.