Eating Challenges & Obturator
Since the beginning of 2025, I’ve had more challenges with eating and swallowing. The good news is that after a year of trying and many attempts, there is a potential solution that has made a noticeable improvement. To achieve this, I’ve seen doctors from University of Chicago Medicine (UCM), Rush, MD Anderson (MDACC) and now University of Illinois Health (UI Health).
Here is the summary version: while I’ve had issues with dry mouth for some time, nasal regurgitation has become a bigger problem. It’s no longer just a nuisance. It has made me more self conscious and mindful about eating and drinking. Food that goes up into my nose will cause me to sneeze and even spices will cause constant sniffling and a runny nose. Worse, liquids can go up and out my nose, which is both a little embarrassing and can stain my clothes.
After two rounds of filler injections to bulk up my palate, I had a prosthetic device called an obturator made. This is like a retainer that physically prevents food from going up my nasopharynx. The obturator was originally made in November 2025 and modified in April 2026. It has had a beneficial impact on my quality of life and being able to enjoy more foods. I now use this nearly every time I eat.
Timeline
23 April 2025: discussed filler procedure with Dr. Maniakas and Dr. Kobayashi at MDACC
9 May 2025: consult with Dr. Gao at UCM re: filler procedure
15 May 2025: consult with Dr. Eggerstedt at Rush re: filler procedure
18 June 2025: in-office filler injection with Dr. Gao
9 July 2025: follow up visit with Dr. Gao
23 September 2025: filler procedure with Dr. Gao - under sedation
8 October 2025: follow up visit with Dr. Gao
10-14 November 2025: obturator fabrication and fitting with Dr. Aponte-Wesson at MDACC
12 November 2025: Modified Barium Swallow Study
27 February 2026: initial visit with Dr. Srivastava at Craniofacial Center at UI Health
8 April 2026: follow up with Dr. Gao, including endoscopy
10 April 2026: modification of obturator by Dr. Srivastava
Swallow Issues & Filler Injections
As mentioned previously, dysphagia - difficulty swallowing - is one of the most concerning long-term side effects of the prior radiation treatments. Specifically, I have velopharyngeal insufficiency (VPI), which is when the soft palate doesn’t completely seal between nasal and oral cavities. In addition to the food issues, it also means that my voice is slightly hyper nasal. I believe most of the issues are related to the first course of treatment in 2018, as that radiation hit a much larger swath of my mouth and neck than the more targeted SBRT in 2023.
Since the start of 2025, my swallowing has worsened in two different ways: a) there is more food residue in my throat, which requires either additional swallowing to get it down or coughing it back out and b) more food and liquid going up my nasal passage. The issues I highlighted in the May 2025 post (“Upward Trends”) continued. The result is that it can be quite uncomfortable to eat certain foods - rice, noodles and broccoli, in particular - almost always go up my nose. In addition, spices can also get into my nose, which causes me to sneeze and have a runny nose while eating. The only way I’ve found to clear this is to blow my nose really hard to expel any food and spies. Further, I have to be conscious of how I drink liquids. The best way is to sit up, tilt my head back and then drink. Drinking while leaning over will surely mean the liquid escapes. Trying to eat or drink too quickly is no longer a viable option. I also have to have napkins/tissue on hand whenever I eat to protect my clothes and to minimize the noticeability of these effects.
The filler injection to the palate was the plan to address the nasal issues. After consulting with new doctors at UCM and Rush, I decided to do the in-office procedure with Dr. Gao at UCM. He is a laryngologist and the co-director of the Voice Center. He has more experience with these sorts of injections, and he recommended starting with an in-office procedure under local numbing. In contrast, Dr. Eggerstedt would have put me under general anesthesia. I appreciated his directness and honesty, but he didn’t seem to have as much specialized experience as Dr. Gao.
One issue that the doctors noted is that the filler material is not a permanent solution. The filler will break down over time, depending on which material is used - anywhere from 3 months to a year. So I would need to get a series of injections over time to achieve the benefit.
The first filler procedure had to wait until 18 June, after our trip to Central Asia. Unfortunately, the procedure did not provide as much benefit as I was hoping. Even while I was in-office, it didn’t go as well as expected. While I’ve had plenty of endoscopies (i.e. a thin tube with a camera going into my nose) with and without numbing and experienced no discomfort, this time was different.
The procedure would involve two people: a technician to insert and hold the scope and Dr. Gao, who could then see where he was working. Since I was getting injected, I had a number of numbing sprays to my nose. I could feel the scope, and it caused a gag reflex. I’m not sure if this was due to the skill of the technician or if it was in a different part of my head that was more sensitive, both, or something else. In any case, this was less than ideal, as it made Dr. Gao’s efforts to inject the filler - Prolaryn Plus (calcium hydroxyapatite) - into my palate much more difficult. He had to pause several times so that I would stop gagging. I needed to be more still for him to finish his work. In the end, he said he injected 0.35ml into three different sites. In addition, after injecting the filler, I kept coughing quite hard, even after the scope was removed. This made it less likely that the filler would hold and remain in place.
First filler that was injected
That night, because my mouth was still a little sensitive from the procedure, I ate chicken soup, i.e. a soft food. However, liquid was still escaping through my nose, so there didn’t seem to be any benefit from the procedure. For food, I first hoped that there would be more noticeable benefit. This did not turn out to be the case - the benefit was minimal to marginal, at best.
My return appointment was originally scheduled for 30 July - 6 weeks following the procedure. But since I didn’t realize any significant benefit, I contacted the team and moved my follow up to 9 July. During that visit, we discussed the next step options, given that the filler injection had such limited benefit. Dr. Gao suggested doing another injection, but this time under sedation. Given the issues with the in-office / local numbing procedure, we thought that the injection while I was completely out would give us the best chance of success. Dr. Gao also said that he typically allows for up to 3 injections to provide benefit - the first injection may not provide the full benefit.
The second procedure was scheduled for mid-August. I was quite looking forward to it, as it’d been over 4 months since the original option was mentioned. Sadly for me, Dr. Gao had to reschedule back to 23 September, so I had to deal with the issues for a further 5 weeks.
The procedure - listed as “CaHA injection augmentation pharyngoplasty” started early in the morning, with a 5:30am check-in to the Center for Care and Discovery at UCM. After a wait in the lobby with other surgical patients, I was taken back to get anesthesia. Needless to say, I don’t remember much of anything between then and when Aiday picked me up a few hours later.
The injection was similar to the in-office procedure in that Dr. Gao and his resident injected 3 separate sites in my nasopharynx with Prolaryn Plus. This is a calcium hydroxyapatite (CaHA) filler that is more durable than a hyaluronic acid filler (e.g. Restylane). Dr. Gao was able to inject nearly the full syringe - 0.95cc - to those sites. However, he said that he couldn’t inject any more to further bulk up the site. The tissue was so scarred from the 2018 radiation that it couldn’t hold any more.
The end result is that this provided only minimal incremental benefit. In the follow up appointment with Dr. Gao on 8 October, we concluded that the scar tissue would prevent the fillers as being the solution to close the gap between my mouth and nose and reduce nasal regurgitation. Additional filler injections would not provide significant benefit, so it was not recommended. He offered two alternatives: a) an obturator and b) a different type of surgery - palatopharyngoplasty with flap reconstruction surgery (aka UPPP). The surgery would move tissue from the back of my throat to the palate. That seemed more risky, so I opted for the obturator. Dr. Gao referred me to Dr. Akanksha Srivastava, a maxillofacial prosthodontist and implantologist at the Craniofacial Center at UI Health.
Obturator - Appointment Scheduling
I called Dr. Srivastava’s office to schedule a consultation. I was hoping that we could make the device before the end of 2025, in part because we had already reached our insurance deductible and out-of-pocket maximums for the year. However, her first appointment was not until February 2026. I was scheduled for a series of 5 appointments over 10 weeks (through April 2026) so that the obturator could be fitted properly. This timing was a let down, as the eating issues were becoming more problematic than a mere nuisance.
I decided to reach out to Dr. Aponte-Wesson, my oral oncologist at MDACC, as I already had appointments for my regular follow up in November 2025. Miraculously, she had availability that week. In addition, she said that if I stayed for the week (Monday-Friday), they could an obturator that week. Extending the trip to Houston was a no-brainer - I could get the device much sooner and without incurring any additional medical bills!
Fitting the Obturator at MDACC
After some travel stress getting to MDACC on Monday, I was glad to be sitting in the oral oncology chair. Dr. Aponte-Wesson and her resident Dr. Chew and a student came to see me. I briefly described my history and where the filler had not worked as expected. One of the things I like most about Dr. Aponte-Wesson is how she radiates positivity and optimism.
I also told her about my scheduled appointment with Dr. Srivastava. She told me to keep the appointment, as they would work together to treat me. I had seen in Dr. Srivastava’s bio that she did a fellowship at MD Anderson. It turns out that Dr. Aponte-Wesson trained Dr. Srivastava and they communicate all the time. So, I knew I would be in good hands!
The first appointment on Monday was relatively straightforward. They took impressions of my mouth - similar to how they made my fluoride trays. The other aspect of fitting was trying to figure out where to put the clamps that would hold the device in place.
On Wednesday, the initial fitting of the obturator took place. When I first placed it in, I didn’t gag, so that was a positive. However, I could not talk clearly, as the obturator was made thicker than expected. Dr. Chew took the obturator out of the room and made a few adjustments, notably making it much thinner all around.
My first impressions of the obturator were quite positive, even though it took some time to get used to it. I was able to realize the benefit right away - I could tell that the obturator was reducing the amount of food that was going up my nose. I could eat things like chips & salsa with less risk. I also enjoyed a great meal at Tatemo, a 1-star Michelin restaurant with a tasting menu focused on Mexican food. I’ll write more about this in a food post about Texas.
I went back on Friday to have Dr. Aponte-Wesson and her team adjust the obturator. Even though it was thinner than the first version, my speech was still less clear with it in. They were able to make it thinner still, which made my enunciation more clear. We iterated through this a few times such that there was a less noticeable difference between having it in vs. having it out when I talk. The other adjustments made the fit better and close some gaps. During the first few meals, I would have food between the obturator and the food of my mouth, which made it an uncomfortable. Also, the device was rocking a little bit when I bit down. The solution to that was to shave off the metal clamp on the front right side. All of those adjustments made for a better fitting and more effective device. I really appreciate Dr. Aponte-Wesson’s excitement for how well it’s working.
I am getting more comfortable eating with it and having it in. There is substantially less food going up my nose. I can also wear it for extended periods - I don’t feel a need to take it as soon as I’m finished eating. That being said, the obturator is not perfect - spices can still cause irritation and liquids will stick come out of nose. The other odd sensation is that I have a hard(er) surface on the roof of my mouth, which I can use to help break down foods. In theory, I guess that could protect against burning the roof of my mouth, but not sure I want to test that too strenuously. (This paragraph was written in November 2025, before the modification, hence the present tense. I thought I would send this post out then, but obviously it’s a bit later.)
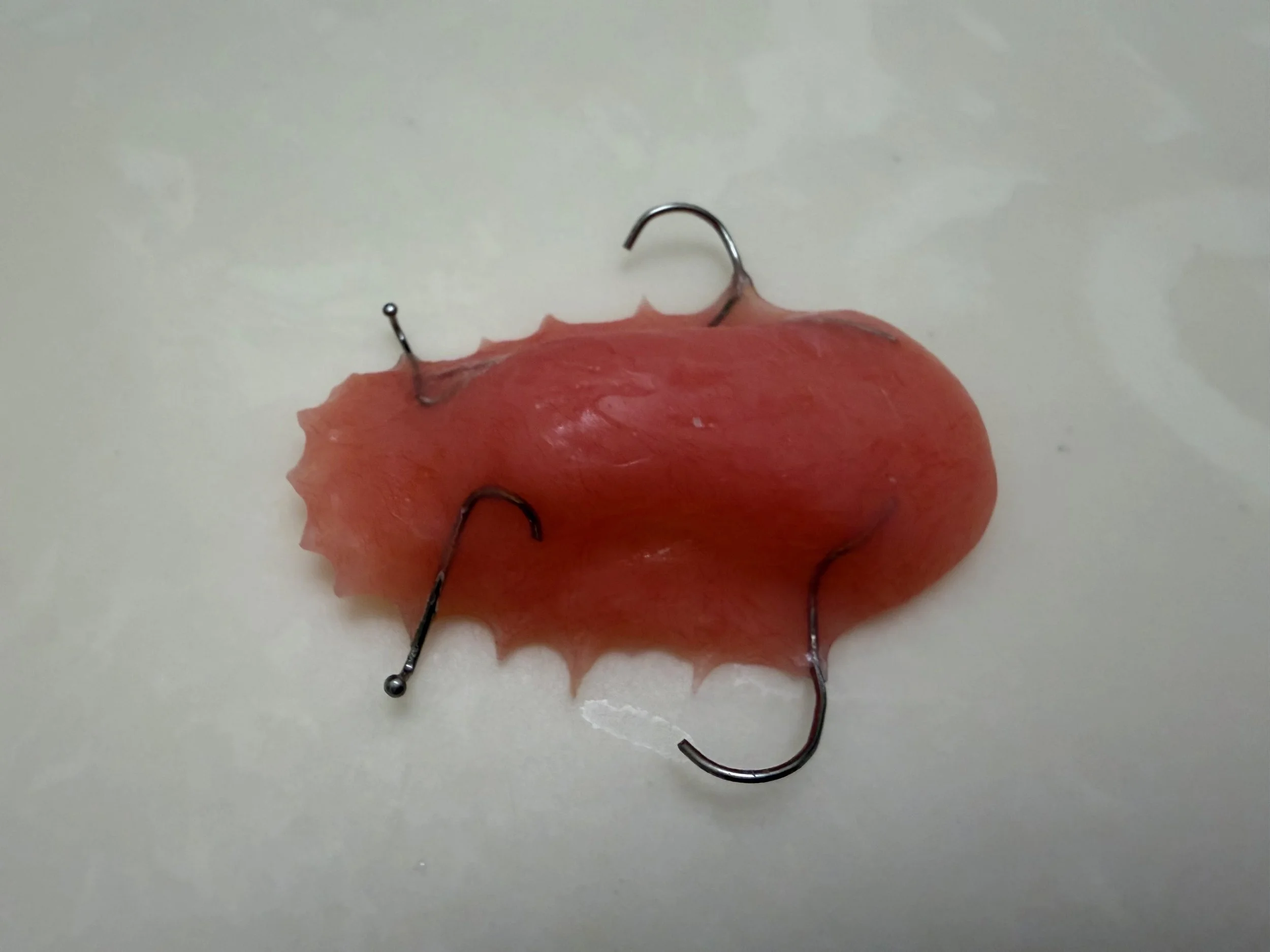
First iteration of the obturator from Wednesday. On Friday, the front right clamp was shaved off and the obturator was thinned down
Modifications at UI Health
I’m glad that I’m now seeing Dr. Srivastava at UI Health. Upon my initial consultation, she told me that not only did she train with Dr. Aponte-Wesson, but that she and Dr. Maniakas (my ENT at MDACC) did their fellowship at the same time, so she also knows him quite well. It’s like my care team is all part of the same cohort! They all share the same positive energy that I very much appreciate.
Following the first fitting in November, I used the obturator for some, though not all, meals and snacks. As time passed, it seemed to become less effective. Dr. Srivastava helped to realize that the initial impressions were taken less than 7 weeks after my September 2025 filler injection. As that filler has broken down, the gap has grown wider, so more and more food was making it through that gap. Dr. Srivastava and I discussed various options for the device, namely modifying it or making a new one. We decided to try to modify it.
In order to do that, I first had to get an endoscopy to see exactly where the deficiency was. Fortunately, I had already scheduled a follow up appointment with Dr. Gao, and he was able to film the endoscopy. He sent the video to Dr. Srivastava. The endoscopy showed that the gap is in the back right corner of my palate.
Dr. Srivastava was able to use this video to modify my obturator by adding some additional material to that area. (I think Dr. Aponte-Wesson had taken a slightly different approach.) With the modifications, the benefits are noticeably better. So much so that I now put in the obturator before nearly every meal. I found a decent case, so I bring it out to meals as well.

Modified obturator - Dr. Aponte-Wesson had shaved off the right front metal brace. UI Health added the extra material in the back to help close the gap
Potential Next Steps
Already, the modified obturator is making a significant improvement. At this point, it is now blocking most all of the food from getting up into my nose. There are some spices that can irritate my nose, but I think that is unavoidable. Similarly, it’s hard to stop all the liquids from coming out my nose. In particular, carbonated beverages (I like to drink sparkling water for my dry mouth) can cause issues. Similarly, certain postures are problematic for both eating and drinking - leaning forward and looking down when eating a bowl of noodles or taking a sip of water at the gym - are positions I now have to avoid.
The good news is that there are some potential improvements still to come. Dr. Gao mentioned the possibility of injecting a thinner filler (e.g. Restylane) into the superficial layer of the palate. He said that this may end up acting like a cyst, so it could be a more permanent solution that won’t degrade. It would also help to further bulk up the palate and ensure the gap remains closed.
In addition, Drs. Aponte-Wesson and Srivastava have mentioned ultimately getting a metal frame obturator. I’m not sure exactly what this looks like, but they said that the current obturator is more like a “training wheels” version to ensure that it provides benefits. The metal frame obturator would be lighter (maybe without the material for the roof of my mouth?) and more durable. However, it does require “countouring” the teeth, i.e. shaping the teeth so the obturator fits better. That’s why they wait to make sure it provides benefits first. They told me the metal obturator would still be removable, just like the current one. Another advantage is that it would make eating feel more natural - there isn’t that layer preventing the roof of my mouth from feeling the temperature and texture of food. Like the additional filler, that’s a decision that doesn’t need to be made today. For now, I can enjoy eating with the plastic obturator - it makes a huge difference to having nothing.
Thank you again for reading all of this and for your support. Since this filler/obturator journey began, we’ve still traveled a lot, including the most recent trip to Singapore and Malaysia in March 2026. There are many travel-related posts that I want to share.